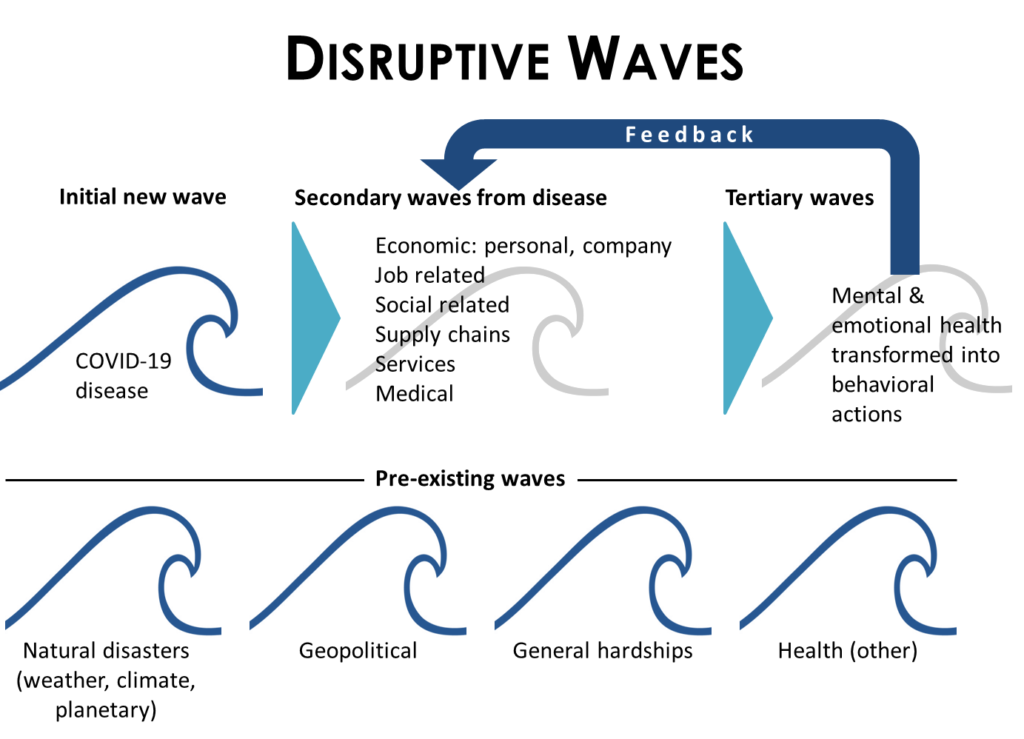
I started looking at COVID-19 as part of a big picture event and now I suggest that we are in the midst of a cluster pandemic event. We all see there are many things going on around us today. It is almost too much for us to understand and manage. It is rocking our world and lifestyle in a nasty way. This is more than COVID-19; it is a cluster of battles in a war for our livelihood.
If we are to win the battle of COVID-19, we need to fight 5 connected pandemics, a cluster pandemic, to survive. We are being crushed by adversity in amounts not witnessed before by our generation. If we beat all 5, we will be better for it individually, as a nation, and as a world.
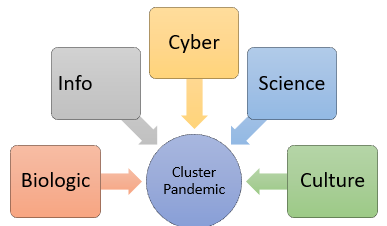
- Biological pandemic (SARS-COV-2 virus)
- Info pandemic
- Cyber pandemic
- Science/Technology pandemic
- Culture pandemic
COVID-19 is a Biological pandemic running rampant in the US as data shows. We need to beat this and there are many initiatives underway to manage it. However, we need to understand all of the connected influences to this Biological pandemic and how they are impacting COVID-19. For one, the Biological pandemic is getting fueled by the Info pandemic and Culture pandemic.
The Info-pandemic is about wide spread misuse of information used to mislead and cause harm to people. This pandemic is also out of control with growing amounts of misinformation and unregulated communications channels in TV news and social media. Anyone can say anything with minimal repercussions and cause harm to people. The average person is not sure who to trust regarding COVID-19 information resulting in unsafe practices that cause an increase in the spread of the virus. The Info pandemic also distracts us from focusing on resolving the biological pandemic through its divisive manner of attack.
The Cyber pandemic is about how hidden, focused attacks are disrupting our way of life. Secure living enables comfort and trust in how we work and play. The Cyber pandemic distracts our focus and impedes our progress on resolving COVID-19 by causing distrust, business disruption, and data integrity issues. Hackers and foreign entities are increasing their battles while becoming more sophisticated and successful in their attacks. Being hidden, it is another pandemic, like the Biological pandemic, that makes it difficult for the average person to understand since most of us can’t see it. We need to depend on, as well as trust, that science will help us find solutions.
The Science pandemic, or Technology pandemic, is about our lack of trust in science.
On the R&D front, the US lags on R&D spending compared to the EU and China. The US has many dependencies on external sources to fuel its innovation. Innovation is the key in finding new ways to defeat biologic threats and to advance our capabilities, An exception to this is Amazon, who reinvests its profits into innovation, new business models, and business growth. Another aspect is our inability to embrace what science tells us as we continue to vandalize the Earth, commit to unimaginable amounts of waste, and refute our impact to the environment while not acknowledging the consequences. R&D is essential to identify solutions to protect our existence,
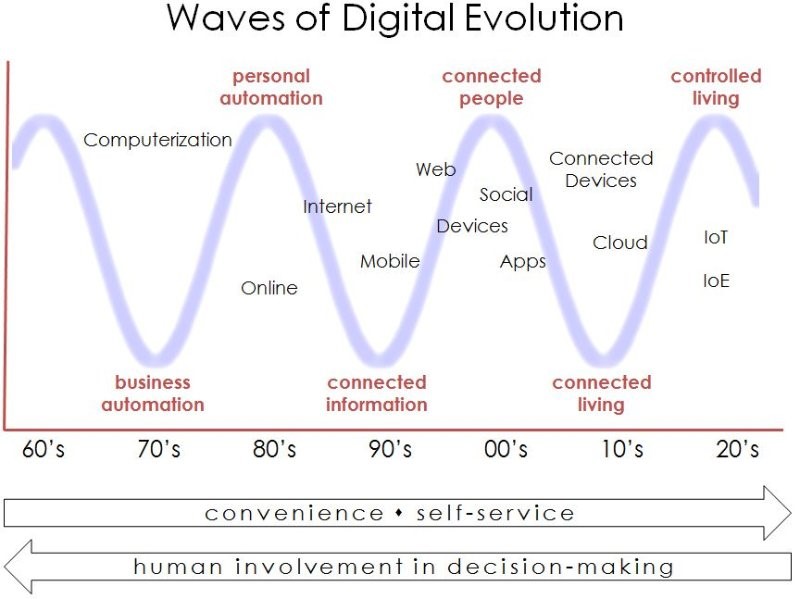
As far as digital, I have seen many businesses, particularly in the healthcare sector, show their reluctance to fully embrace digital methods with speed, investment, and sponsorship. The Culture pandemic is partly due to a lack of digital adoption as well since a digital mindset is imperative for digital initiatives to flourish.
The Culture pandemic is about our mindset as individuals and as a people. It is about how we think and behave while guided by strong leadership and focused direction. For example, in the US, we live in a ME culture that focuses on personal desires while celebrating our individual successes while other countries live as a WE culture that work as one to the benefit of many. Our way of thinking limits our ability to act in unity to combat COVID-19 and all the other pandemics. The Culture pandemic impacts the Biological pandemic in many of us by our wanting not to be told what to do and not conforming to precautions recommended by medical experts. This is exacerbated with some leaders providing conflicting information on what to do – the Info pandemic.
What a formidable task that lies before us. No wonder we have been having so much trouble in the COVID-19 battle – it is a war and not just one battle. If we want to manage COVID-19, we need to manage all 5 pandemics together since they are connected and impact one another. We have the ability to win this and our humanity depends on it. History will see this time as us battling the granddaddy of all pandemics – a 5 pandemic cluster event – so it is a time to rethink this and attack with vigilance.